

Vakharia, VN;
Smith, L;
Tahir, Z;
Sparks, R;
Ourselin, S;
Tucker, S;
Thompson, D;
(2021)
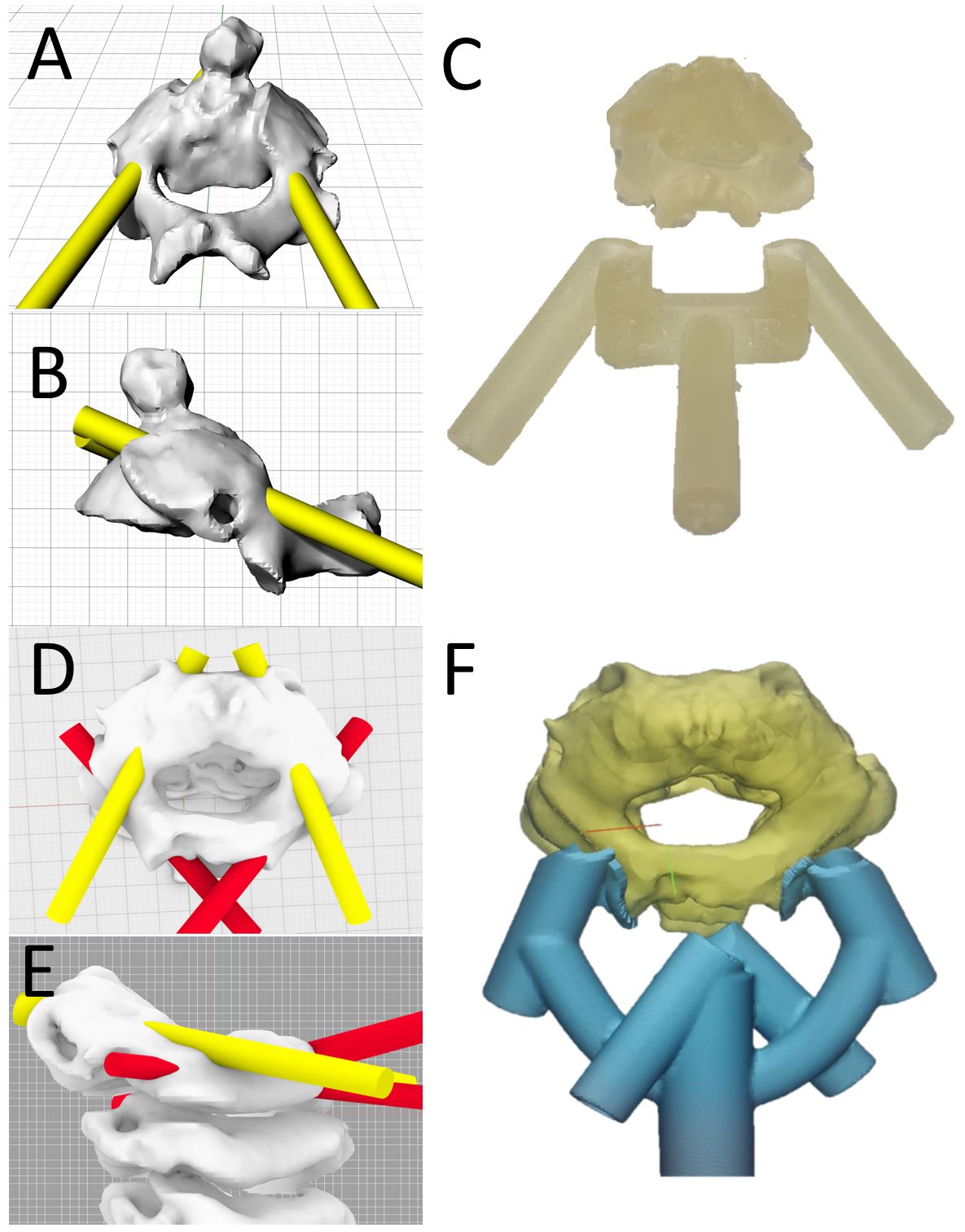
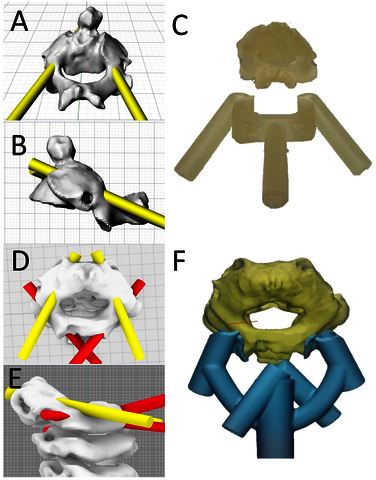
Occipitocervical instrumented fixation utilising patient-specific C2 3D-printed spinal screw trajectory guides in complex paediatric skeletal dysplasia.
Child's Nervous System
, 37
pp. 2643-2650.
10.1007/s00381-021-05260-2.

Preview |
Text (Accepted version)
Vakharia_CNS_3DSSTG_amended.pdf - Accepted Version Download (143kB) | Preview |
Preview |
Image (Figure 1)
Figure_1.tif - Accepted Version Download (1MB) | Preview |
![[thumbnail of Figure 2]](https://discovery-pp.ucl.ac.uk/10132744/8/Figure_2.JPG) 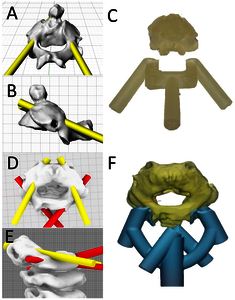 Preview |
Image (Figure 2)
Figure_2.JPG - Accepted Version Download (181kB) | Preview |
Preview |
Image (Figure 3)
Figure_3.tif - Accepted Version Download (474kB) | Preview |
Preview |
Image (Figure 4)
Figure_4.tif - Accepted Version Download (2MB) | Preview |
Preview |
Image (Figure 5)
Figure_5.tif - Accepted Version Download (1MB) | Preview |
Abstract
Purpose: Instability of the craniocervical junction in paediatric patients with skeletal dysplasia poses a unique set of challenges including anatomical abnormalities, poor bone quality, skeletal immaturity and associated general anaesthetic risks. Instrumented fixation provides optimal stabilisation and fusion rates. The small vertebrae make the placement of C2 pedicle screws technically demanding with low margins of error between the spinal canal and the vertebral artery. Methods: We describe a novel clinical strategy utilising 3D-printed spinal screw trajectory guides (3D-SSTG) for individually planned C2 pedicle and laminar screws. The technique is based on a pre-operative CT scan and does not require intraoperative CT imaging. This reduces the radiation burden to the patient and forgoes the associated time and cost. The time for model generation and sterilisation was < 24 h. Results: We describe two patients (3 and 6 years old) requiring occipitocervical instrumented fixation for cervical myelopathy secondary to Morquio syndrome with 3D-SSTGs. In the second case, bilateral laminar screw trajectories were also incorporated into the same guide due to the presence of high-riding vertebral arteries. Registration of the postoperative CT to the pre-operative imaging revealed that screws were optimally placed and accurately followed the predefined trajectory. Conclusion: To our knowledge, we present the first clinical report of 3D-printed spinal screw trajectory guides at the craniocervical junction in paediatric patients with skeletal dysplasia. The novel combination of multiple trajectories within the same guide provides the intraoperative flexibility of potential bailout options. Future studies will better define the potential of this technology to optimise personalised non-standard screw trajectories.

{kind=link}
{kind=link}
Archive Staff Only
 |
View Item |